HARTFORD, CT, July 23, 2022 /24-7PressRelease/ — It is often said that a knee is simply not a knee post-surgery. As is the case with so many aspects of our lives and bodies that we take for granted. We scarcely realize how much pressure a joint like the knee must endure to keep us moving smoothly and pain-free. Of course, this is until something goes wrong and we need surgery to correct it.
While knee surgeries are sometimes the best option, they have come a long way. Improvements have been primarily due to the changes in medical knowledge and available technologies.
How ROM Technologies is Changing the Game
As stated prior, technology has done wonders to improve the results we experience from undergoing knee surgery. Much of this is due to changes in post-surgery knee recovery technology. ROMTech is a leading organization in pre-op and post-op knee surgery recovery.
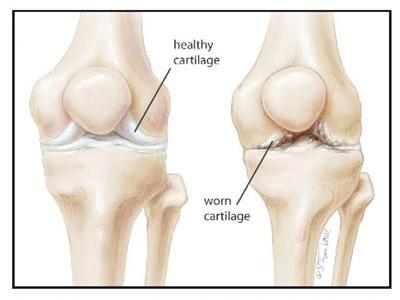
Knee replacement is the most popular surgical option. In the past, this would leave recipients with stiff knees that would not help them move or function as efficiently as they desired. Today, the opposite is true.
Today, athletes can undergo knee replacement surgery and, with strategic rehabilitative work, find that they can work their way back to peak capacity. Thanks to leading medical technology organizations, having a knee rehabilitation resource helps ensure that patients can recover as quickly and efficiently as possible with smooth, pain free movement.
Knee replacement surgery no longer means that a sporting career has to end or that daily life has to be significantly hampered. Thanks to ROMTech’s work in producing high-quality joint replacement material, their work is not only limited to knees.
ROM Technologies PortableConnect actually used in both knee and hip patients rehabilitation as well. This makes sense, as a debilitatingly injured or arthritic hip can impact the knees negatively and vice versa. It makes sense that these key features of the lower extremities are considered in tandem.
How to Get Started Working with ROMTech
Since their PortableConnect device enables knee and hip recovery it is easy to see what their focus is on, improving quality of life. Sometimes people with knee and hip issues may be concerned with having to do a procedure.
However, the advancements in ROM Technologies help ensure that higher-quality replacements help reduce the likelihood of the same. As such, they encourage anyone who may need replacement surgery (irrespective of age or even profession) to have it done sooner rather than later.
—
Press release service and press release distribution provided by http://www.24-7pressrelease.com